Belated results from drug and alcohol PbR recovery pilots
Regular readers and those of you with long memories may remember when payment by results was heralded as the future of the commissioning of public services in the UK. PbR has fallen out of favour in the last few years with the much-publicised difficulties of the Work Programme and Troubled Families project.
PbR has also been out of the news because it was always celebrated as an evidence-based approach (providers only being paid if they achieved outcomes) and the evaluation reports of a number of high profile PbR projects weren’t published, leading most commentators to presume that this was because their findings were not positive.
However, over the last month PbR has returned to the media spotlight. Last month (27 July 2017), the MoJ published the outcomes from the second (and final cohort), of the Peterborough Prison resettlement PbR project – which found that the (now discontinued) service reduced re-offending by 9%.
Two days ago (15 August 2017), researchers published an evaluation of the drug and alcohol PbR recovery pilots. Readers should note that this is not the formal, final evaluation promised by the Department of Health for April 2015, but does provide detailed information on the outcomes of the 8 pilot areas compared with all other drug treatment services in England.
The report
Entitled “Does paying service providers by results improve recovery outcomes for drug misusers in treatment in England?”, and written by Andrew Jones, Mattias Pierce, Matt Sutton, Thomas Mason & Tim Millar, the evaluation was based on analysis of all drug misuse treatment that was provided in England between 2010 and 2014 and included over 300,000 spells of treatment.
The study compared key outcomes in the eight pilot areas that tried the Payment by Results approach with outcomes in the areas that did not.
Key findings – a mixed bag
The key findings make for interesting reading.
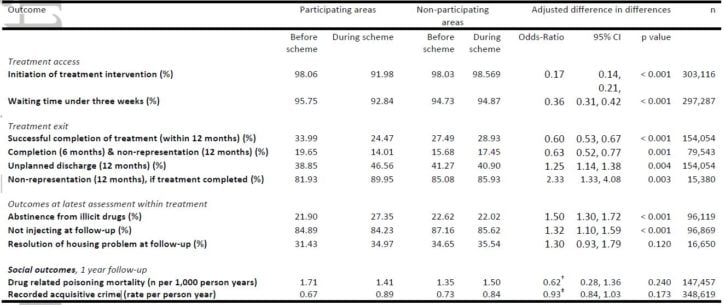
On the one hand, clients in the PBR pilot areas, waited longer to access treatment, were more likely to experience an unplanned discharge from treatment and were less likely to successfully complete their treatment, or complete without re-presentation for further treatment. The proportion of service users who successfully completed drug misuse treatment (within twelve months of its inception) actually went down in pilot areas, from 34% to 24%, but increased from 27% to 29% in the other (non-PbR) areas.
Conversely, the scheme was associated with service users reporting abstinence from illicit substances and alcohol (up from 22% to 27% in PbR areas, down slightly, from 23% to 22%, in the other areas) and with a lower rate of injecting whilst in treatment. Further, among the subset of clients who did successfully complete treatment, those in participating areas were less likely than those in non-participating areas to return to treatment within one year.
The authors also highlight an issue which I have always considered a design fault of the pilot schemes; that concern about potential gaming of the system introduces an additional layer of expensive bureaucracy (the assessment and referral system known as LASARS) which also delays treatment since the initial assessment is for the purpose of setting payment tariffs rather than promoting recovery.
One of the most interesting findings to me, not commented on in the paper but shown in a table, was that the rate of recorded acquisitive crime by people in treatment increased in the pilot areas noticeably from 0.67 proven reoffences per person per year to 0.89. This worrying increase was only not highlighted in the commentary because the rate also jumped (if less substantially) in the non-PbR areas from 0.73 to 0.84 per person per year.
Conclusions
Dr Tim Millar, who led the impact evaluation said:
Drug treatment services already work extremely hard to improve the lives of service users who often have problems that are extraordinarily complex and deeply entrenched.
Perhaps it shouldn’t come as a great surprise that we did not find clear cut evidence that the scheme produced the benefits that were intended.