
Yesterday (7 June 2018), the European Monitoring Centre for Drugs and Drug Addiction published its annual report on drugs in Europe (of which more next week) and 30 individual country reports. This blog post focuses on the UK report and highlights facts and issues which I found interesting; I hope you do too.
Continued fall in drug offences
After increasing between 2006/07 and 2010/11, the number of arrests for drug law offences has decreased in recent years. In 2015/16, approximately 115 377 court convictions and police cautions for drug offences were reported in England, Wales, Scotland and Northern Ireland. Of the offences in which the drug involved was recorded (in England, Wales and Scotland), 57 % were cannabis related, 20 % were cocaine related (excluding crack cocaine) and 11 % were heroin related.
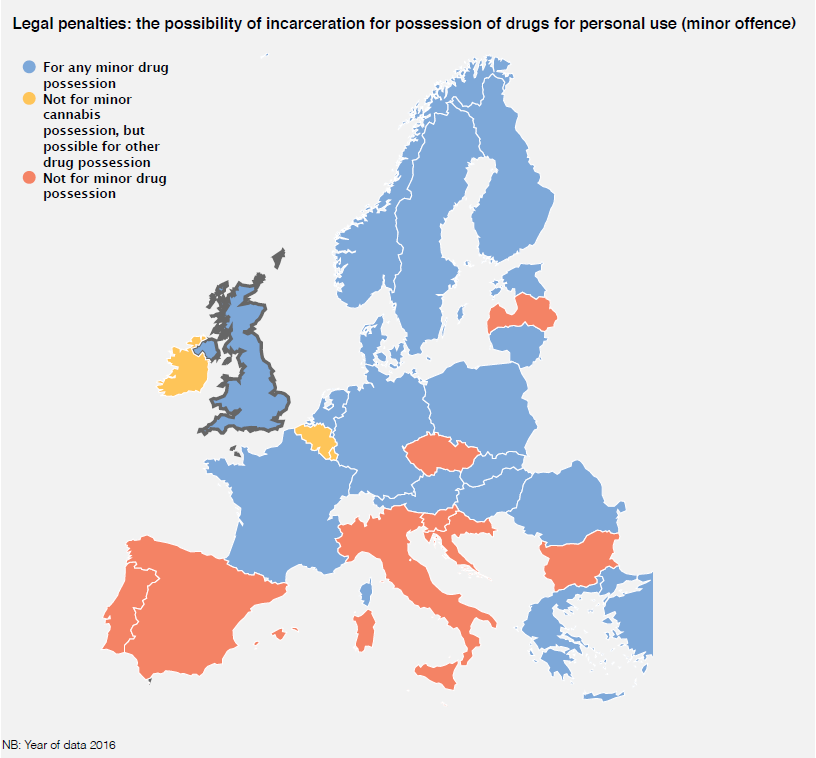
UK punishments out of step with Europe
UK citizens can still be imprisoned for minor offences of possession of any drug, unlike much of the rest of Europe (See graphic below):
Prevalence and trends
Overall drug use in the United Kingdom has declined from the level seen 10 years ago, remaining stable in the past three years. Because of its relatively high prevalence, cannabis has been a substantial driver of this overall trend. Cannabis remains the most commonly used illicit drug, while powder cocaine is the most prevalent stimulant in the United Kingdom and the second most prevalent drug overall. MDMA/ecstasy is the next most commonly reported stimulant. In general, MDMA users are younger than cocaine and amphetamines users.
According to the Crime Survey for England and Wales, among 16- to 34-year-old young adults, cannabis use declined between 2006 and 2013, but has since levelled off. Cocaine use decreased between 2008 and 2010 and has been relatively stable since. Having previously declined, the level of reported MDMA use has returned to a level broadly similar to that seen around 10 years ago. Prevalence of new psychoactive substances (NPS) in general population surveys is low in comparison with the main traditional drugs. Mephedrone is the only stimulant NPS to have become established alongside traditional substances among recreational drug users within the general population. However, the prevalence of use of this drug has fallen since 2010/11.
Drug-related infectious diseases
There is a long-term declining trend in new HIV cases linked to injecting drug use in the United Kingdom, and the rate of injecting-related HIV remains low. In 2015, an outbreak of HIV occurred among people who inject drugs
(PWID) in Glasgow, with 50 new HIV cases reported in Scotland, which was more than double the average number of new HIV cases detected annually in the period 2006-2014. In 2016, Scotland registered a total of 36 new HIV cases. The data from Unlinked Anonymous Monitoring (UAM) in England, Wales and Northern Ireland also indicate that the estimated prevalence of HIV among PWID has been in decline.
It is estimated that the majority of all hepatitis C virus (HCV) infection cases in the United Kingdom are a result of injecting drug use. The prevalence of HCV infection among PWID remains relatively high and has changed little in recent years; in 2016, almost half of all PWID were estimated to be HCV positive. There are geographical variations in HCV prevalence across the United Kingdom, with the prevalence of HCV (and other blood-borne viruses) being lower in Northern Ireland than in the rest of the United Kingdom. The prevalence of HCV antibodies among recent initiates to injecting drug use has remained fairly stable over the past decade.
Drug-induced deaths and mortality
In 2015, the United Kingdom reported a record number of drug-related deaths, indicating an increasing trend since 2012. Because of elays in the registration of deaths, the number of deaths in 2016 is not yet known, but statistics published on the number of deaths registered in 2016 in particular in Scotland suggest that a further increase in the UK total is expected. Opioids (primarily heroin, but also methadone) were involved in the majority of deaths (almost 9 in 10), and other drugs commonly associated with deaths from illicit substance use include benzodiazepines, cocaine (frequently in combination with heroin) and amphetamines.
The presence of multiple psychoactive substances in drug-related deaths is becoming more common in the United Kingdom. Males made up almost three quarters of drug-related deaths cases in 2015, and the mean age at time of death was 42 years. The average age of those dying has risen every year since 2006.
Treatment provision
Around 245 000 clients received drug treatment in England and Wales in 2016. Approximately half of them presented for treatment in the United Kingdom during 2016, one third of whom had never been treated previously. Just under half of all clients presenting for treatment in this year were primary opioid users. Cannabis is the most frequently reported primary drug among first treatment presentations, and has increased in importance in recent years.
The number of opioid users prescribed OST has decreased slightly since the 2010 peak, although it remains above 2006 levels. In 2016, 138 422 patients received OST in England and Wales. The number of new clients entering treatment for heroin use decreased for several years but now seems to have stabilised.






3 responses
I am struggling to reconcile the text under the heading “UK punishments out of step with Europe” with the graphic… Am I reading this wrong? The graphic shows eight countries in red as “Not for minor drug possession” (Portugal, Spain, Italy, Slovenia, Croatia, Czech Republic, Bulgaria and Latvia), three in orange as “Not for minor cannabis possession, but possible for other drug possession” (Ireland, Belgium and Luxembourg) and then 17 in blue representing “For any minor drug possession” – including the UK.
Hi T
Fair point, “much” is rather over-egging the pudding although more countries are moving away from incarceration for minor drug possession.
Thanks for your interest
Russell
First of all i’m not a drug user apart from alcohol and smoking on a small administration, however at a late age i tried Cannabis, the supply made me dizzy so i thought i’ll try my own,
i grew a couple of plants, while harvesting them it made me feel sick even more and gave away the proceeds and never touched it since.
What is the big deal with Cannabis, why not allow those to have a supply of quality like i grew rather than have a supply from gangs that murder and force prostitution.
I don’t get it from politicians that we should be in prohibition like the USA was with booze, the consequences are far worse.
Apparently those whom consumed my plant thought it was great and wanted more, all it did was chill them out they said, that’s all they wanted is to chill out, where is the harm?
Please don’t reply that it’s a corridor to much harder drugs!