
The 2018 Global State of Harm Reduction is the sixth edition of this biennial report from Harm Reduction International, and the most comprehensive ever with input from over 100 harm reduction practitioners, academics, advocates and activists from around the world.
It finds that, since the last report in 2016, the global harm reduction response has effectively stalled. Overdose, HIV and hepatitis C crises continue, among myriad health and social problems related to drug use and drug policy, yet many countries are neglecting them. Of the estimated 15.6 million people who inject drugs worldwide, over half live with hepatitis C, and nearly 1 in 5 live with HIV.
The 2018 report has a broader scope than its predecessors and contains information on:
- The number of people who inject drugs and the number of people imprisoned for drug use (where data is available).
- Needle and syringe programmes (NSP), opioid substitution therapy (OST), HIV and hepatitis C and TB testing and treatment for people who use drugs, in both the community and in prisons.
- The harm reduction response for people who use amphetamine-type stimulants, cocaine and its derivatives, and new psychoactive substances.
- Drug-checking in nightlife settings.
- Harm reduction for women who use drugs.
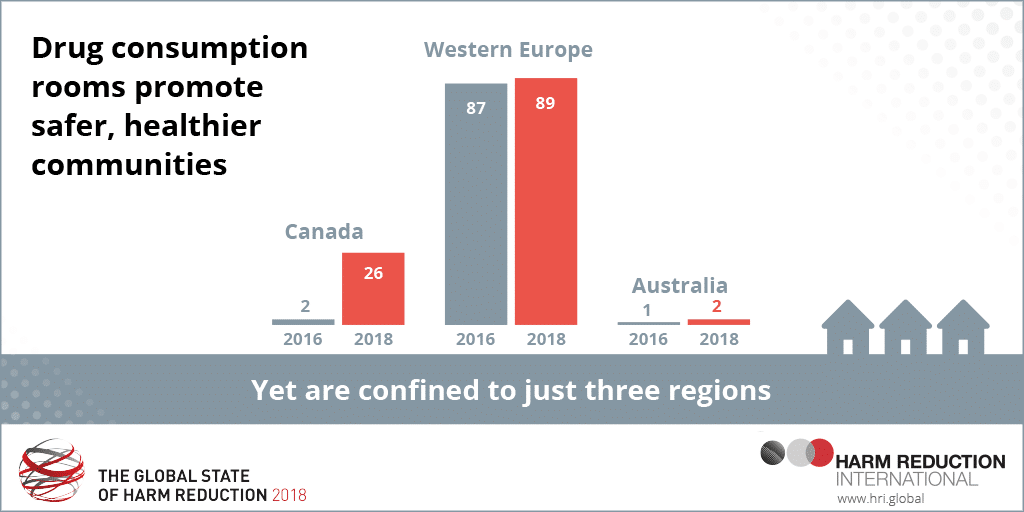
- Drug consumption rooms.
- Drug-related mortality and morbidity and the overdose response, as well as naloxone peer distribution in the community and naloxone provision in prisons.
- Developments and regressions in funding for harm reduction.

Developments
The number of countries providing opioid substitution therapy (OST) rose slightly from 80 to 86 in the last two years, while the number of drug consumption rooms (DCRs) globally increased from 90 to 117 in the same period. However, OST provision is well short of what is required for an effective public health response, and DCRs are confined to just 11 countries in Western Europe, Canada and Australia.
Alongside mapping access across nine regions to HIV and hepatitis C treatment, and naloxone (a medicine to
reverse opioid overdose), the report provides the first global mapping of harm reduction for amphetamine type
stimulants (ATS) and cocaine, such as drug-checking, safer smoking kits, and housing programmes.
There are approximately 35 million ATS users worldwide, yet programmes for these drugs are severely
underdeveloped, the report finds. Drug checking programmes exist in five regions (Western Europe, Latin
America, North America, Oceania and Eurasia), but are largely confined to nightlife and festival settings.
Harm reduction in prison
Harm reduction in prisons remains in a worse state than in the community. Despite the fact that up to 90% of
people who inject drugs may be incarcerated at some point in their lives, only 10 countries implement NSP in
prisons, and 54 provide OST. Prisons are high-risk environments for the transmission of blood-borne infections
and tuberculosis, and harm reduction interventions are effective in mitigating this risk.
A notable development since 2016 has been the rapid emergence of new psychoactive substance (NPS) use in prisons. In particular, the use of synthetic cannabinoids in prisons is an issue of concern in Germany, Sweden and the United Kingdom. At least 58 deaths in British prisons have been attributed in part to NPS use, for example through psychotic episodes, suicide and/or drug poisoning.
Access to harm reduction services in prisons varies significantly between and within countries in Europe. For example, services appear to be widespread in Spain, with service coverage similar in prison to in the community.Conversely, no harm reduction services are available in Turkish prisons.
NSP provision in prisons is inadequate, with only four countries in Western Europe providing such programmes. These are: Spain (all prisons), Switzerland (15 out of 117 prisons), Luxembourg (one of two prisons) and Germany (one female prison in Berlin) – there has never been needle and syringe provision in a UK prison.
Despite the accepted high risks of (often fatal) overdose in the period immediately after release from prison, the distribution of naloxone to prisoners on release only takes place in four European countries (Denmark, France, Norway and the UK) and its implementation in the UK is very patchy, with good distribution in Scotland and much more variable accessibility for prison leavers in England and Wales.




