Meta-analysis
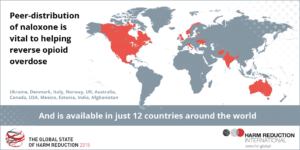
Drug-related deaths globally are increasing year on year, with the largest proportion of these being opioid-related. The opioid antagonist naloxone distributed for take-home use (‘Take-Home Naloxone (THN)’) has been championed as one method of tackling this public health crisis, however to be effective it must be available at an opioid overdose. Ownership and carriage are therefore fundamental to THN success. A new research study conducted by a Scottish team aimed to assess the prevalence of ownership and carriage of THN internationally among people who use drugs (PWUD).
The researchers, Gillian Burton, Andrew McAuley , Joe Schofield, Alan Yeung, Catriona Matheson & Tessa Parkes, undertook a systematic review and meta-analysis of international studies looking at the prevalence of take-home naloxone ownership and what they have termed “carriage”. Carriage simply means whether people regularly have their naloxone with them – clearly if someone has a naloxone kit at home, it is of little use if someone overdoses anywhere else.
The researchers identified ten relevant studies of sufficient quality. They found good levels of ownership of THN – an average of 57% of at risk people who inject drugs – but a much lower level of carriage: 20%.
The researchers identify a number of reasons why people who have naloxone don’t take it with them:
- Aspects of product design (e.g. bulky packaging) which make THN difficult to carry;
- Stigma or identification as a person who uses drugs as a result of THN carriage; and
- Police perceptions or criminal repercussions if THN is perceived to be drug-related paraphernalia.
- The fact that people mainly inject drugs at home and therefore don’t carry naloxone with them. Of course, this also means that the person would not have naloxone with them to use on a drug-injecting peer outside the home.

The researchers identify a wide range of implications from their study for policy makers and practitioners including: addressing the barriers to carrying naloxone listed above and widening the distribution points of THN to include a number of key agencies who regularly have contact with people who inject drugs including GPs, accident and emergency departments and general medical services.
The researchers also recommend that in light of the COVID-19 pandemic, widening of access is needed given the relative decrease in face- to-face support and the concurrent increased risk to PWUD. They advocate that novel methods of distribution including postal THN distribution and online training, which work around COVID-19 restrictions, should also be used and advertised widely in all forums accessed by PWUD.
Finally, the researchers note that there are no commonly agreed definitions for ownership and carriage of THN and the adoption of these would make the evidence base much more reliable and useful.
Nevertheless, it is clear that the rates of THN ownership and, in particular, carriage are much lower than they could be to make a significant impact on reducing the numbers of drug-related deaths from opioid overdoses. The World Health Organisation recommends targets of 90% of people receiving overdose risk and management training being given THN and 90% of those who are supplied with naloxone carrying it with them on a regular basis.