The Forward Trust has just published a new briefing setting out a model for driving up the numbers of opiate using prisoners who leave prison with naloxone, the anti-opioid overdose medication.
The rise in drug-related deaths
The number of drug-related deaths in England and Wales is at an all-time high, with 3,756 deaths in 2017. 53% of these deaths involved an opioid. Deaths involving fentanyl – a synthetic opioid that is 50 times more potent than heroin – rose by 29% in 2017. There does not currently appear to be widespread demand for fentanyl-laced heroin in the UK and it is hard to tell from sight alone whether a batch of heroin contains fentanyl. This suggests that heroin users may be consuming fentanyl unknowingly.
People leaving prison are at the highest risk of overdose and drug-related death in the first weeks following release. This is likely due to reduced tolerance to heroin, increased purity of drugs compared to those used in prison and the tendency of some released prisoners to return to previous drug use patterns.
Increasing the uptake of Take Home Naloxone (THN) amongst opioid users leaving prison (and in the community)
can help reduce the number of drug-related deaths amongst this high risk population.
What is Take Home Naloxone (THN)?
THN is a prescription-only drug that can reverse the effects of opioids such as heroin, morphine, buprenorphine,
codeine, methadone, opium, pethidine and fentanyl. It does not affect non-opioid drugs such as crack cocaine, ecstasy
and cannabis (among others). THN can reverse the reduced breathing rate caused by an opioid overdose and therefore
prevent death.
THN is supplied in a kit that includes a syringe pre-filled with naloxone and needles. Once a needle has been twisted onto the syringe, it can be injected into the muscle. It takes approximately 2-5 minutes for naloxone to have an effect which lasts for 20-30 minutes. More than one dose can be given if someone returns to an overdose state after the effects have worn off.
Since October 2015, drug services in prisons and the community can supply THN to service users without a prescription. Pharmacists who provide services such as needle exchange programmes can also supply THN. This means that any opioid users at risk of overdose, as well as their family, friends and peers, can obtain naloxone to save a life in an emergency.
Despite being a policy priority for some years, it has so far proved difficult to get decent levels of take up of THN on release. Where THN programmes are available in prison, there are a number of factors contributing to low take-up by opioid users leaving prison. Service providers in prisons with a high number of individuals on remand or with a high churn have a limited window of opportunity to offer THN. Opioid service users who are not receiving opioid substitution therapy are less likely to be offered THN, perhaps due to providers focusing THN distribution on those they believe to be at highest risk of overdose upon release. Finally, service users may be offered THN, but refuse it because they believe they will not use opioids again and therefore think they have no need for it.
Maximising take-up
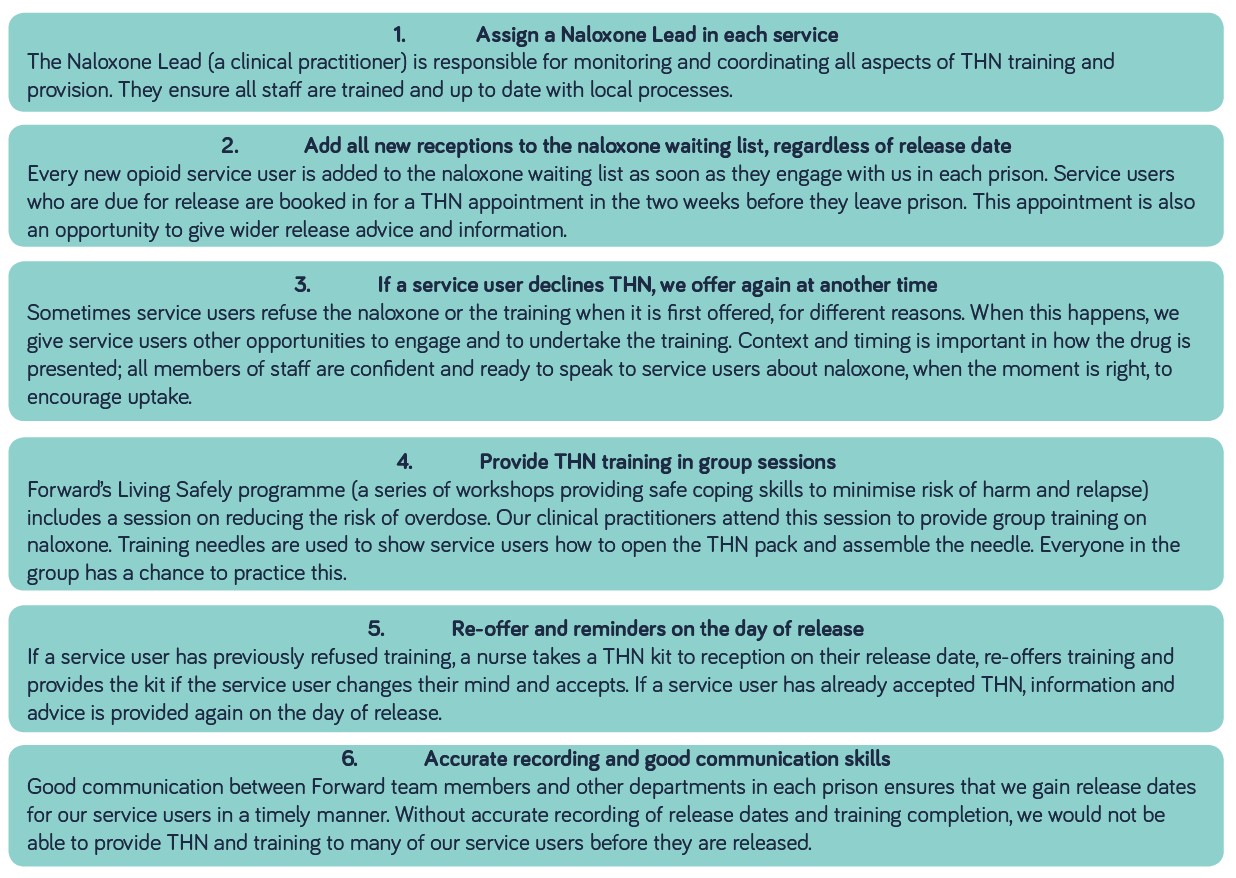
Forward have developed the a six-step best practice process to increase the number of service users accepting THN ahead of their return to the community set out in the graphic below:
Impact
The comprehensive approach to THN described above was first implemented by Forward in HMP Lewes in 2018. Within a year of implementing the initiative, the number of opioid service users at HMP Lewes who were released with a naloxone kit was at 48%, 4 times higher than the national average.
Results were almost as impressive at the other prisons where Forward provides clinical treatment service (only qualififed medical staff can prescribe naloxone), with an average of 42% opioid service users across 11 prisons taking Naloxone home.
It is to be hoped that as THN rates increase, awareness of naloxone among prison staff and opiate using prisoners grows and more and more prisoners will take home naloxone, saving more lives.





