A very mixed picture
By way of a change today, I am actually summarising a piece of research undertaken by myself. Over the last two months I’ve been researching the experiences of opiate using offenders seeking substitute prescribing (methadone or buprenorphine – usually known as Subutex or “Subbies”) in prison and on release.
Interestingly, service users had very mixed experiences with some finding access to a script easier than in the community while others received no help despite being on a prescription in the community prior to being sent to prison.
I used two main methods to gain service user views. First, an online survey was completed by 102 opiate users who had been in an English or Welsh prison in the last two years. Opiate using prisoners were identified and recruited by 10 peer researchers trained, supervised and supported by the Revolving Doors Agency.
Analysis of the survey data informed the second stage of the research study; a focus group with nine individuals with recent experience of Opioid Substitute Treatment (OST) in prison.
To put the research into context, a recent FOI request revealed that 22,514 prisoners received pharmacological interventions for opiate use in 2016.
Access to medication in prison
Survey respondents were first asked whether they wanted medication for their opiate dependency; whether they wanted methadone or buprenorphine and whether they wanted to be on a maintenance or reducing prescription.
As can be seen from the chart below; 95% of respondents did want medication, with a majority wanting a maintenance prescription and a majority also preferring methadone to buprenorphine.

The respondents who did not want methadone or buprenorphine stated they wanted dihydrocodeine and benzodiazepine (“DFs and sleepers”).
Respondents were then asked: “If you wanted medication, did you get it?” and were given a choice of five options which reflected ease of access:
- Yes – I was offered medication
- Yes – I asked for medication and got it easily
- Yes – I asked for medication and had to work hard to get it
- Yes – I got some medication, but not what (or as much) as I wanted
- No (I did not get medication)
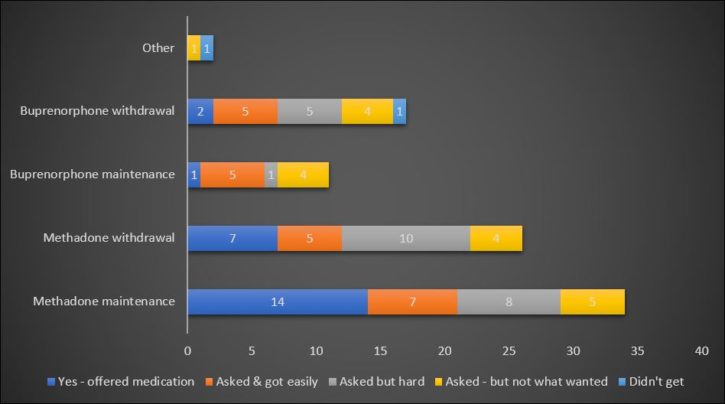
The vast majority (88/94 = 94%) respondents did receive at least some medication with varying degrees of ease of access:
It was harder for those wanting buprenorphine to get what they wanted than those who wanted methadone.
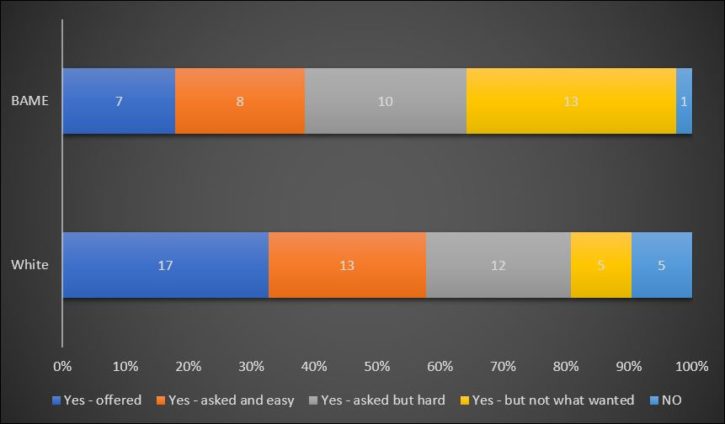
It was also more difficulty for prisoners from a Black and Minority Ethnic (BAME) background to get what they wanted:
Access to some form of OST in prison was often better than in the community. However, there was rarely any user choice about either substance or whether OST was prescribed on a maintenance or withdrawal basis. There was a common experience that anyone serving a sentence of longer than three months (equating to 6 weeks in custody) would be place on a withdrawal prescription. Several participants were unable to access medication on their first day in prison, especially if they arrived late in the day.
Several individuals reported that even when existing prescriptions were confirmed with a community physician, these were regarded as an initial bargaining position by prison prescribers who typically halved dosages of medications including opioid substitutes and benzodiazepines.
Several individuals talked about the prescribing process as being like a factory production line with no consideration of their emotional or psychological needs and a focus on prescribing minimal levels of opioid substitutes. Details of prescribing regimes were often not shared and several individuals reported going to collect their daily medication only to be told their prescription had ended,
Many participants shared the view that prescribers were increasingly reluctant to prescribe certain medications because of their diversion and re-sale. This applied particularly to gabapentin and buphenorphine and, to a lesser extent, methadone.
Continuity of care on release
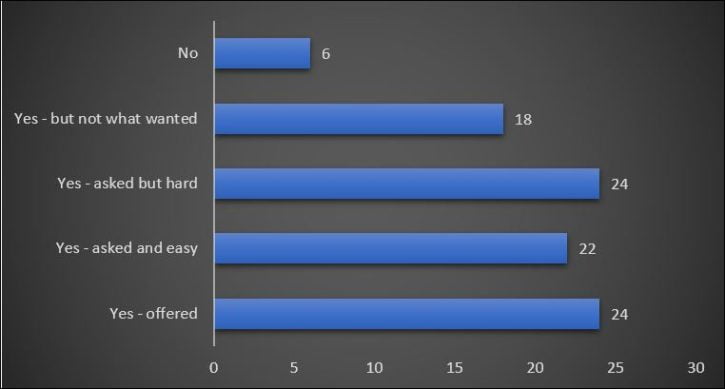
I also enquired whether, if they received medication in prison, service users were offered a continuing prescription on release. Again, there was a very mixed experience with just over half (52%) either offered medication on release or asked for it and secured it easily. However, almost two fifths (38%) either received no medication or did not get the type or as much as they wanted.
Several individuals who did receive a continuing prescription commented that they received sufficient substitute medication to last between one and three days before seeing their drug worker in the community. Four respondents reported difficulties in getting seen promptly by their community agency and running out of substitute medication.
Quality of care
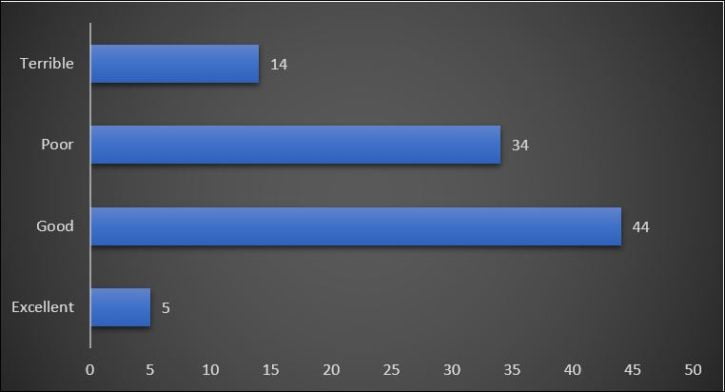
Although the survey focused primarily on the provision of OST in prison, I also asked service users to rate their overall satisfaction with the help they were given for their drug problem inside on a simple four-point scale:
- Excellent, I really got the help I needed
- Good, not perfect, but overall I got a lot of help
- Poor, there were some key things I needed which I just didn’t get
- Terrible – I didn’t get any help at all
Opinions were almost equally split with just over half (49/97 = 51%) rating help as good as excellent and 49% rating it as poor or terrible:
Suggested improvements
Finally I asked both survey respondents and focus group participants to nominate the “one thing which would most improve help for heroin users in prison”. The responses from those taking the survey were categorised into the ten main themes listed below in order of popularity:
- More support available (17 respondents)
- Improved staff skills and attitudes (10)
- Listening to prisoners/better communication (9)
- Reduced availability of drugs, particularly New Psychoactive Substances (7)
- Recovery wings/prisons (6)
- Treatment passports – documents recording existing medications to accompany individuals between prison and community (5)
- Consistent approach between prisons/minimum standards (5)
- More peer mentors (4)
- Better continuity between prison and community (3)
- Narcotics Anonymous meetings (3)
Focus group participants were also asked to nominate the key issues they would like to see improved in prison drug treatment and highlighted four concerns:
- Access to support for people serving short sentences (no fewer than six individuals reported being offered access to a peer mentor or drug treatment programme in the week prior to release).
- Reliable access to a proper withdrawal programme (participants were prepared to “trade” a rapid withdrawal for an assurance that they would receive some support).
- A medical passport system where people could receive the same prescription that they were getting in the community – at least initially.
- Help with support on release, particularly with accommodation without which they felt it was impossible to even attempt to reduce or control their drug use.
Conclusion
Despite many criticisms, there was an acknowledgement of considerable improvement in prison OST over the last 10-15 years with service users equally split between those who rated their prison drug treatment experience as excellent and good and those who rated it poor or terrible.
I have also summarised the research in the infographic below. If you can’t see the infographic on your device, please click here.
You can download the full report here. If you’d like a copy of the infographic in PDF format, please: Email me.
[The research was supported by an educational grant from Martindale Pharma which had no input into the design of the research, nor the analysis and publication of the results.]
Blog posts in the drug and alcohol category are kindly sponsored by Breaking Free Group which has developed a powerful and adaptable digital health platform which targets the underlying psychological and lifestyle factors that drive addictive behaviours. Breaking Free has no editorial influence on the contents of this site.